Does Minoxidil Affect DHT? Every Study, and What They Actually Show
No human study shows minoxidil lowers DHT, and the lab studies contradict each other. Here is every study on whether minoxidil is a DHT blocker, and why it does not matter.
No human study shows minoxidil lowers DHT, and the lab studies contradict each other. Here is every study on whether minoxidil is a DHT blocker, and why it does not matter.
Does minoxidil affect DHT? It is one of the most common questions in hair loss, and the honest answer has two layers that point in the same direction.
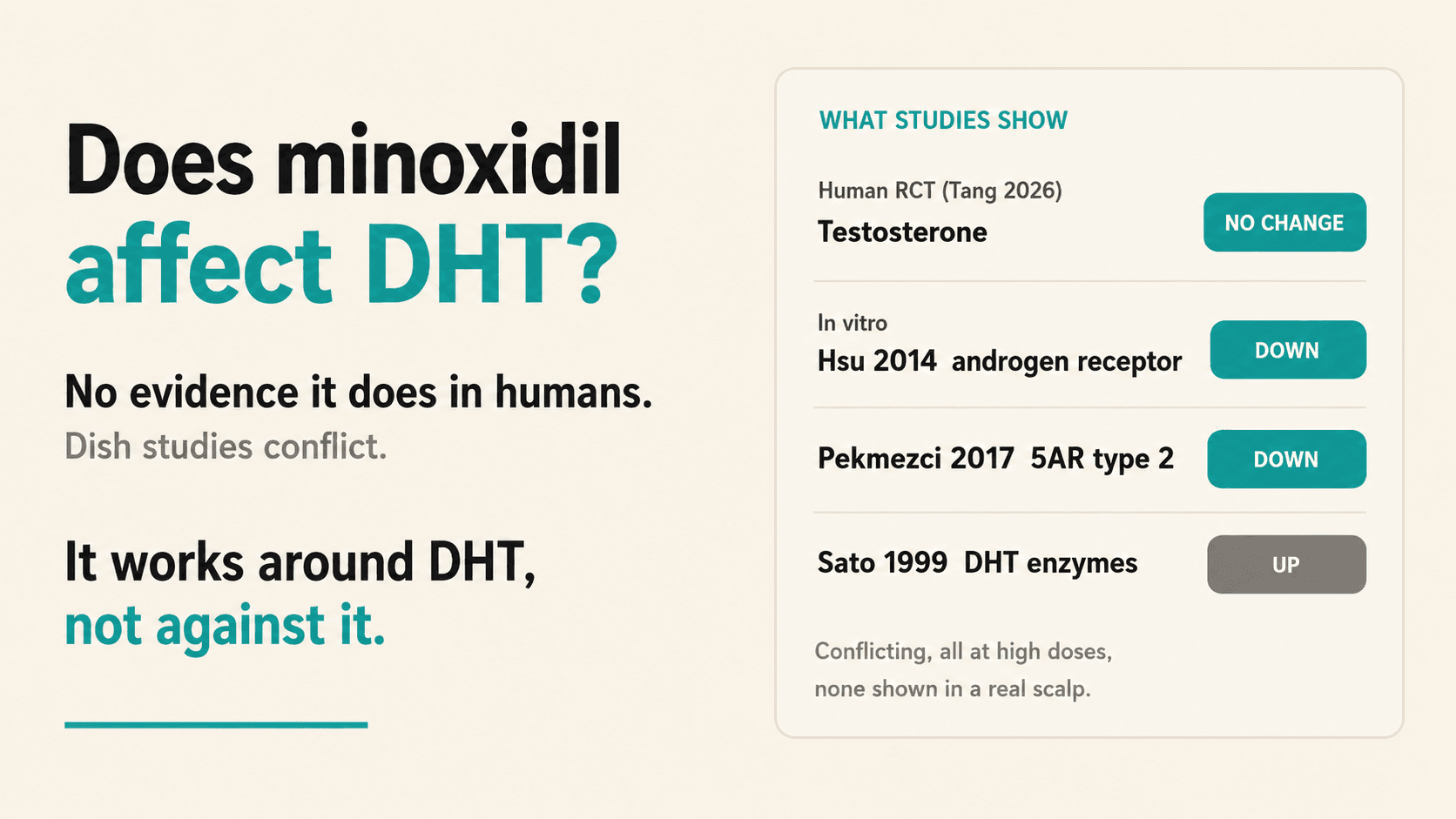
The short answer: In humans, there is no evidence minoxidil affects DHT. The best clinical data, a 2026 randomized controlled trial, found minoxidil grew hair with no change in testosterone at all (Tang 2026). In the lab, a handful of cell studies show minoxidil can touch the androgen machinery, but they point in opposite directions: some say it lowers androgen activity, one says it raises the enzymes that build DHT, and a brand-new one suggests it may even hit the estrogen receptor. None has been reproduced in a living scalp. Minoxidil is not a DHT blocker. It works downstream, around DHT, not against it. That is exactly why it pairs so well with a drug that does block DHT.
No. There is no human evidence that minoxidil lowers the dihydrotestosterone (DHT) in your blood or your scalp.
This is the single most important thing to understand about the drug, because it sits right next to finasteride and dutasteride on nearly every hair-loss shelf, and those two do the opposite job.
DHT is the hormone at the center of male pattern baldness. In genetically susceptible follicles, DHT binds the androgen receptor and slowly miniaturizes the hair, cycle after cycle, until the follicle produces something thin and short instead of a full terminal hair (Kaufman 1998). Reduce DHT and you slow that process at the source.
That is what 5-alpha-reductase inhibitors do. Finasteride blocks the type II 5-alpha-reductase enzyme that converts testosterone into DHT, and in scalp tissue it drops local DHT by roughly 40% (Olsen 2006). Dutasteride blocks both enzyme types and pushes that number higher.
Minoxidil does none of this.
The cleanest human answer comes from a 2026 randomized, double-blind, placebo-controlled trial (Tang 2026). It studied sublingual minoxidil in transgender people receiving full-dose testosterone therapy, a group in which a 5-alpha-reductase inhibitor would have been a problem, because lowering DHT interferes with masculinization. Minoxidil was chosen precisely because it is not hormonal.
The result: minoxidil significantly improved hair count (+15.7 hairs/cm2 in the midfrontal scalp versus placebo, p = 0.03) and had "no effect on testosterone concentrations." It grew hair without moving the androgen it was measured against.
Older work points the same way. The canonical mechanism paper (Messenger and Rundegren 2004), the single most-cited review of how minoxidil works, explains its action entirely through the hair cycle and the opening of potassium channels, and never invokes androgens at all. And notably, in more than fifty years of use, no trial has ever measured a change in serum or scalp DHT caused by minoxidil. The clinical picture is consistent: minoxidil is hormonally neutral.
Minoxidil is a prodrug. On its own, it does almost nothing to a hair follicle.
The active molecule is not minoxidil at all. It is minoxidil sulfate, and your follicle makes it on site. An enzyme in the outer root sheath called SULT1A1 (sulfotransferase 1A1) converts the drug into its sulfated, active form right where it is needed (Buhl 1990; Messenger and Rundegren 2004). How much of that enzyme you have varies from person to person, and it predicts how well you respond, which is why two people on the identical dose can get very different results (Roberts 2014).
Once minoxidil sulfate is made, the honest answer is that we still do not know exactly how it grows hair. What we do know is the first step: minoxidil sulfate opens ATP-sensitive potassium channels (Messenger and Rundegren 2004). Everything else appears to happen downstream of that event, and none of it is hormonal.
One myth is worth killing here, because it is everywhere. Minoxidil is a vasodilator, so people assume it grows hair by increasing blood flow to the scalp. That is almost certainly not the mechanism. Plenty of drugs increase scalp blood flow and do nothing for hair, and the old vasodilation theory has largely been set aside. Minoxidil taken orally was originally a blood-pressure drug, but its hair-growth effect does not track with what it does to blood vessels. Minoxidil does not work by improving circulation.
What does seem to matter, downstream of the potassium channels, are its effects on the follicle itself:
The key honesty point: the exact chain from an open potassium channel to a thicker hair has never been fully worked out. Messenger and Rundegren even note that it has not been clearly shown these potassium channels are expressed in the hair follicle at all. Minoxidil works. Precisely how, past that first step, is still an open question. What is clear is what it does not do. It does not act on DHT, and it does not simply work by boosting blood flow.
This is where a lot of internet claims go off the rails.
In the laboratory, minoxidil genuinely can interfere with the androgen system. But the studies do not agree with each other, and that disagreement is the whole point. Here is the complete set.
Hsu and colleagues (2014) ran a detailed set of biochemistry experiments and found that minoxidil binds directly to the androgen receptor. They measured the binding strength at a Kd of 2.6 micromolar, solved a co-crystal structure of minoxidil sitting in the receptor's ligand-binding pocket, showed that it suppressed the receptor's transcriptional activity, and demonstrated that it slowed the growth of DHT-driven prostate cancer cells. The same suppression showed up in human hair dermal papilla cells. This points toward less androgen activity.
Pekmezci and Turkoglu (2017) went at the enzyme end of the pathway. They treated a human keratinocyte cell line (HaCaT) with minoxidil and measured 5-alpha-reductase type 2 gene expression. Minoxidil knocked it down to about a fifth of baseline (0.22 fold, p < 0.0001). They titled the paper "Minoxidil Acts as an Antiandrogen." This also points toward less DHT.
So far, so tidy. Two studies, both suggesting minoxidil dampens the androgen pathway. Then the third study turns the story upside down.
Sato and colleagues (1999) measured testosterone metabolism in cultured dermal papilla cells and found the opposite direction. In cells from balding scalp, minoxidil increased 17-beta-hydroxysteroid dehydrogenase activity by nearly 40% (p < 0.001) and slightly increased 5-alpha-reductase activity. Those are the enzymes that build DHT. In this experiment, minoxidil looked like it could make more androgen locally, not less. The authors were honest about the uncertainty: "Whether such modification of testosterone metabolism in dermal papilla cells of balding scalp by minoxidil is related to its therapeutic effect remains unknown."
And there is a brand-new wrinkle. Elzaghir and colleagues (2026) asked whether minoxidil might touch the other half of the sex-hormone axis, and reported preliminary evidence that it may act as a partial agonist of estrogen receptor alpha. This is early, single-group, and explicitly labeled preliminary, but it widens the picture: minoxidil's molecular reach may not be limited to the androgen receptor at all.
Read any single one of these papers quickly and it sounds like a smoking gun. Read all of them together and the smoking gun disappears.
Here is the honest read.
First, the studies disagree on direction. One set says minoxidil lowers androgen activity (Hsu 2014, Pekmezci 2017), one says it raises the DHT-building enzymes (Sato 1999), and the newest says it may act on estrogen instead (Elzaghir 2026). You cannot build a clinical claim on a literature that points four different ways.
Second, all of these were cells in a dish, exposed to minoxidil at micromolar concentrations chosen by the experimenter. That is a very different setting from a living human scalp treated with a topical or a low oral dose.
Third, and most important, nobody has shown that any of this changes DHT in a real person. Blood and scalp DHT do not drop the way they do on finasteride, the one clean human hormone readout (testosterone, in Tang 2026) showed no change, and not a single clinical outcome for minoxidil depends on an anti-androgen effect. Its efficacy is fully explained by the growth-phase mechanisms above.
So the cell studies are real, and they are a fascinating hint that minoxidil's molecular reach is broader than we thought. They may matter for future drug design or for cancer research, which is what Hsu's team was chasing. But they are not evidence that the minoxidil in your medicine cabinet is quietly acting as a DHT blocker. It is not, at least not in you.
It does not.
Baldness is a two-part problem. There is the signal that tells the follicle to shrink, and there is the follicle's actual response to that signal. DHT is the signal. Miniaturization is the response.
A 5-alpha-reductase inhibitor works on the first half. It quiets the signal. Minoxidil works on the second half. It props the follicle up regardless of what the signal is saying.
That is why the strongest evidence-based hair-loss regimens combine them. You lower the DHT hitting the follicle and you push the follicle to grow at the same time. Two mechanisms, no overlap.
Minoxidil was never supposed to be a DHT blocker. Asking it to lower your DHT is asking it to do a job it was never built for, when it is already excellent at a different one.
A few practical takeaways follow directly from the biology:
No. There is no human evidence that minoxidil lowers DHT in your blood or scalp at the doses used for hair loss. Lowering DHT is the job of finasteride and dutasteride, which block the 5-alpha-reductase enzyme. Minoxidil works through a separate, non-hormonal mechanism (Messenger and Rundegren 2004).
No. Minoxidil is not a DHT blocker. It does not reduce DHT or block it from reaching the follicle in any clinically demonstrated way. It stimulates hair growth downstream of DHT by extending the growth phase and raising local growth factors, not by acting on hormones.
Because two lab studies found minoxidil can bind the androgen receptor (Hsu 2014) and lower 5-alpha-reductase type 2 gene expression in cultured cells (Pekmezci 2017). But a third study found the opposite, with minoxidil raising the DHT-building enzymes in dermal papilla cells (Sato 1999). These are conflicting petri-dish results at high concentrations, none shown to change DHT in a real scalp.
The best evidence says no. In a 2026 randomized controlled trial, minoxidil had no effect on testosterone concentrations (Tang 2026). It is hormonally neutral in humans. A separate 2026 lab study reported minoxidil might interact with the estrogen receptor, but that finding is preliminary and unconfirmed (Elzaghir 2026).
Almost certainly not. Minoxidil is a vasodilator, but many drugs increase scalp blood flow without growing hair, and the old vasodilation theory has been set aside. Its hair effect appears to run downstream of potassium-channel opening, through growth factors like VEGF and prolonged anagen. The exact chain is still not fully known.
They are commonly combined precisely because they work through different mechanisms: finasteride lowers DHT while minoxidil pushes the follicle to grow. Whether the combination is right for you is a decision to make with a clinician, since finasteride and oral minoxidil are used off-label for hair loss in the US.
This blog is for educational purposes only and is not medical advice. Minoxidil, finasteride, and dutasteride used for androgenetic alopecia involve off-label prescribing decisions in the US that should be made with a licensed clinician. Topical minoxidil is FDA approved for hair loss; oral and sublingual minoxidil are not. Nothing here is a claim that any specific product treats, cures, or prevents any condition. Talk to your dermatologist before changing any treatment.
Buhl AE, Waldon DJ, Baker CA, Johnson GA. Minoxidil sulfate is the active metabolite that stimulates hair follicles. J Invest Dermatol. 1990;95(5):553-557. PMID: 2230218.
Messenger AG, Rundegren J. Minoxidil: mechanisms of action on hair growth. Br J Dermatol. 2004;150(2):186-194. PMID: 14996087. DOI: 10.1111/j.1365-2133.2004.05785.x
Roberts J, Desai N, McCoy J, Goren A. Sulfotransferase activity in plucked hair follicles predicts response to topical minoxidil in the treatment of female androgenetic alopecia. Dermatol Ther. 2014;27(4):252-254. PMID: 24773771.
Lachgar S, Charveron M, Gall Y, Bonafe JL. Minoxidil upregulates the expression of vascular endothelial growth factor in human hair dermal papilla cells. Br J Dermatol. 1998;138(3):407-411. PMID: 9580790. DOI: 10.1046/j.1365-2133.1998.02115.x
Sato T, Tadokoro T, Sonoda T, Asada Y, Itami S, Takayasu S. Minoxidil increases 17 beta-hydroxysteroid dehydrogenase and 5 alpha-reductase activity of cultured human dermal papilla cells from balding scalp. J Dermatol Sci. 1999;19(2):123-125. PMID: 10098703. DOI: 10.1016/s0923-1811(98)00048-6
Hsu CL, Liu JS, Lin AC, Yang CH, Chung WH, Wu WG. Minoxidil may suppress androgen receptor-related functions. Oncotarget. 2014;5(8):2187-2197. PMID: 24742982. DOI: 10.18632/oncotarget.1886
Pekmezci E, Turkoglu M. Minoxidil Acts as an Antiandrogen: A Study of 5alpha-reductase Type 2 Gene Expression in a Human Keratinocyte Cell Line. Acta Dermatovenerol Croat. 2017;25(4):271-275. PMID: 30064598.
Tang GT, Leemaqz S, Bhoyrul B, et al. Treatment of androgenetic alopecia in transgender people receiving testosterone therapy with sublingual minoxidil: a randomized, double-blind, placebo-controlled clinical trial. J Am Acad Dermatol. 2026 (online ahead of print). PMID: 42140362. DOI: 10.1016/j.jaad.2026.05.020
Elzaghir R, Collins KC, Abdulshafi A, et al. Minoxidil May be a Partial Agonist of Estrogen Receptor Alpha. MicroPubl Biol. 2026. PMID: 42318156. DOI: 10.17912/micropub.biology.002173
Olsen EA, Hordinsky M, Whiting D, et al. The importance of dual 5alpha-reductase inhibition in the treatment of male pattern hair loss: results of a randomized placebo-controlled study of dutasteride versus finasteride. J Am Acad Dermatol. 2006;55(6):1014-1023. PMID: 17110217. DOI: 10.1016/j.jaad.2006.05.007
Kaufman KD, Olsen EA, Whiting D, et al. Finasteride in the treatment of men with androgenetic alopecia. J Am Acad Dermatol. 1998;39(4 Pt 1):578-589. PMID: 9777765.
No human study shows minoxidil lowers DHT, and the lab studies contradict each other. Here is every study on whether minoxidil is a DHT blocker, and why it does not matter.
Does minoxidil affect DHT? It is one of the most common questions in hair loss, and the honest answer has two layers that point in the same direction.
The short answer: In humans, there is no evidence minoxidil affects DHT. The best clinical data, a 2026 randomized controlled trial, found minoxidil grew hair with no change in testosterone at all (Tang 2026). In the lab, a handful of cell studies show minoxidil can touch the androgen machinery, but they point in opposite directions: some say it lowers androgen activity, one says it raises the enzymes that build DHT, and a brand-new one suggests it may even hit the estrogen receptor. None has been reproduced in a living scalp. Minoxidil is not a DHT blocker. It works downstream, around DHT, not against it. That is exactly why it pairs so well with a drug that does block DHT.
No. There is no human evidence that minoxidil lowers the dihydrotestosterone (DHT) in your blood or your scalp.
This is the single most important thing to understand about the drug, because it sits right next to finasteride and dutasteride on nearly every hair-loss shelf, and those two do the opposite job.
DHT is the hormone at the center of male pattern baldness. In genetically susceptible follicles, DHT binds the androgen receptor and slowly miniaturizes the hair, cycle after cycle, until the follicle produces something thin and short instead of a full terminal hair (Kaufman 1998). Reduce DHT and you slow that process at the source.
That is what 5-alpha-reductase inhibitors do. Finasteride blocks the type II 5-alpha-reductase enzyme that converts testosterone into DHT, and in scalp tissue it drops local DHT by roughly 40% (Olsen 2006). Dutasteride blocks both enzyme types and pushes that number higher.
Minoxidil does none of this.
The cleanest human answer comes from a 2026 randomized, double-blind, placebo-controlled trial (Tang 2026). It studied sublingual minoxidil in transgender people receiving full-dose testosterone therapy, a group in which a 5-alpha-reductase inhibitor would have been a problem, because lowering DHT interferes with masculinization. Minoxidil was chosen precisely because it is not hormonal.
The result: minoxidil significantly improved hair count (+15.7 hairs/cm2 in the midfrontal scalp versus placebo, p = 0.03) and had "no effect on testosterone concentrations." It grew hair without moving the androgen it was measured against.
Older work points the same way. The canonical mechanism paper (Messenger and Rundegren 2004), the single most-cited review of how minoxidil works, explains its action entirely through the hair cycle and the opening of potassium channels, and never invokes androgens at all. And notably, in more than fifty years of use, no trial has ever measured a change in serum or scalp DHT caused by minoxidil. The clinical picture is consistent: minoxidil is hormonally neutral.
Minoxidil is a prodrug. On its own, it does almost nothing to a hair follicle.
The active molecule is not minoxidil at all. It is minoxidil sulfate, and your follicle makes it on site. An enzyme in the outer root sheath called SULT1A1 (sulfotransferase 1A1) converts the drug into its sulfated, active form right where it is needed (Buhl 1990; Messenger and Rundegren 2004). How much of that enzyme you have varies from person to person, and it predicts how well you respond, which is why two people on the identical dose can get very different results (Roberts 2014).
Once minoxidil sulfate is made, the honest answer is that we still do not know exactly how it grows hair. What we do know is the first step: minoxidil sulfate opens ATP-sensitive potassium channels (Messenger and Rundegren 2004). Everything else appears to happen downstream of that event, and none of it is hormonal.
One myth is worth killing here, because it is everywhere. Minoxidil is a vasodilator, so people assume it grows hair by increasing blood flow to the scalp. That is almost certainly not the mechanism. Plenty of drugs increase scalp blood flow and do nothing for hair, and the old vasodilation theory has largely been set aside. Minoxidil taken orally was originally a blood-pressure drug, but its hair-growth effect does not track with what it does to blood vessels. Minoxidil does not work by improving circulation.
What does seem to matter, downstream of the potassium channels, are its effects on the follicle itself:
The key honesty point: the exact chain from an open potassium channel to a thicker hair has never been fully worked out. Messenger and Rundegren even note that it has not been clearly shown these potassium channels are expressed in the hair follicle at all. Minoxidil works. Precisely how, past that first step, is still an open question. What is clear is what it does not do. It does not act on DHT, and it does not simply work by boosting blood flow.
This is where a lot of internet claims go off the rails.
In the laboratory, minoxidil genuinely can interfere with the androgen system. But the studies do not agree with each other, and that disagreement is the whole point. Here is the complete set.
Hsu and colleagues (2014) ran a detailed set of biochemistry experiments and found that minoxidil binds directly to the androgen receptor. They measured the binding strength at a Kd of 2.6 micromolar, solved a co-crystal structure of minoxidil sitting in the receptor's ligand-binding pocket, showed that it suppressed the receptor's transcriptional activity, and demonstrated that it slowed the growth of DHT-driven prostate cancer cells. The same suppression showed up in human hair dermal papilla cells. This points toward less androgen activity.
Pekmezci and Turkoglu (2017) went at the enzyme end of the pathway. They treated a human keratinocyte cell line (HaCaT) with minoxidil and measured 5-alpha-reductase type 2 gene expression. Minoxidil knocked it down to about a fifth of baseline (0.22 fold, p < 0.0001). They titled the paper "Minoxidil Acts as an Antiandrogen." This also points toward less DHT.
So far, so tidy. Two studies, both suggesting minoxidil dampens the androgen pathway. Then the third study turns the story upside down.
Sato and colleagues (1999) measured testosterone metabolism in cultured dermal papilla cells and found the opposite direction. In cells from balding scalp, minoxidil increased 17-beta-hydroxysteroid dehydrogenase activity by nearly 40% (p < 0.001) and slightly increased 5-alpha-reductase activity. Those are the enzymes that build DHT. In this experiment, minoxidil looked like it could make more androgen locally, not less. The authors were honest about the uncertainty: "Whether such modification of testosterone metabolism in dermal papilla cells of balding scalp by minoxidil is related to its therapeutic effect remains unknown."
And there is a brand-new wrinkle. Elzaghir and colleagues (2026) asked whether minoxidil might touch the other half of the sex-hormone axis, and reported preliminary evidence that it may act as a partial agonist of estrogen receptor alpha. This is early, single-group, and explicitly labeled preliminary, but it widens the picture: minoxidil's molecular reach may not be limited to the androgen receptor at all.
Read any single one of these papers quickly and it sounds like a smoking gun. Read all of them together and the smoking gun disappears.
Here is the honest read.
First, the studies disagree on direction. One set says minoxidil lowers androgen activity (Hsu 2014, Pekmezci 2017), one says it raises the DHT-building enzymes (Sato 1999), and the newest says it may act on estrogen instead (Elzaghir 2026). You cannot build a clinical claim on a literature that points four different ways.
Second, all of these were cells in a dish, exposed to minoxidil at micromolar concentrations chosen by the experimenter. That is a very different setting from a living human scalp treated with a topical or a low oral dose.
Third, and most important, nobody has shown that any of this changes DHT in a real person. Blood and scalp DHT do not drop the way they do on finasteride, the one clean human hormone readout (testosterone, in Tang 2026) showed no change, and not a single clinical outcome for minoxidil depends on an anti-androgen effect. Its efficacy is fully explained by the growth-phase mechanisms above.
So the cell studies are real, and they are a fascinating hint that minoxidil's molecular reach is broader than we thought. They may matter for future drug design or for cancer research, which is what Hsu's team was chasing. But they are not evidence that the minoxidil in your medicine cabinet is quietly acting as a DHT blocker. It is not, at least not in you.
It does not.
Baldness is a two-part problem. There is the signal that tells the follicle to shrink, and there is the follicle's actual response to that signal. DHT is the signal. Miniaturization is the response.
A 5-alpha-reductase inhibitor works on the first half. It quiets the signal. Minoxidil works on the second half. It props the follicle up regardless of what the signal is saying.
That is why the strongest evidence-based hair-loss regimens combine them. You lower the DHT hitting the follicle and you push the follicle to grow at the same time. Two mechanisms, no overlap.
Minoxidil was never supposed to be a DHT blocker. Asking it to lower your DHT is asking it to do a job it was never built for, when it is already excellent at a different one.
A few practical takeaways follow directly from the biology:
No. There is no human evidence that minoxidil lowers DHT in your blood or scalp at the doses used for hair loss. Lowering DHT is the job of finasteride and dutasteride, which block the 5-alpha-reductase enzyme. Minoxidil works through a separate, non-hormonal mechanism (Messenger and Rundegren 2004).
No. Minoxidil is not a DHT blocker. It does not reduce DHT or block it from reaching the follicle in any clinically demonstrated way. It stimulates hair growth downstream of DHT by extending the growth phase and raising local growth factors, not by acting on hormones.
Because two lab studies found minoxidil can bind the androgen receptor (Hsu 2014) and lower 5-alpha-reductase type 2 gene expression in cultured cells (Pekmezci 2017). But a third study found the opposite, with minoxidil raising the DHT-building enzymes in dermal papilla cells (Sato 1999). These are conflicting petri-dish results at high concentrations, none shown to change DHT in a real scalp.
The best evidence says no. In a 2026 randomized controlled trial, minoxidil had no effect on testosterone concentrations (Tang 2026). It is hormonally neutral in humans. A separate 2026 lab study reported minoxidil might interact with the estrogen receptor, but that finding is preliminary and unconfirmed (Elzaghir 2026).
Almost certainly not. Minoxidil is a vasodilator, but many drugs increase scalp blood flow without growing hair, and the old vasodilation theory has been set aside. Its hair effect appears to run downstream of potassium-channel opening, through growth factors like VEGF and prolonged anagen. The exact chain is still not fully known.
They are commonly combined precisely because they work through different mechanisms: finasteride lowers DHT while minoxidil pushes the follicle to grow. Whether the combination is right for you is a decision to make with a clinician, since finasteride and oral minoxidil are used off-label for hair loss in the US.
This blog is for educational purposes only and is not medical advice. Minoxidil, finasteride, and dutasteride used for androgenetic alopecia involve off-label prescribing decisions in the US that should be made with a licensed clinician. Topical minoxidil is FDA approved for hair loss; oral and sublingual minoxidil are not. Nothing here is a claim that any specific product treats, cures, or prevents any condition. Talk to your dermatologist before changing any treatment.
Buhl AE, Waldon DJ, Baker CA, Johnson GA. Minoxidil sulfate is the active metabolite that stimulates hair follicles. J Invest Dermatol. 1990;95(5):553-557. PMID: 2230218.
Messenger AG, Rundegren J. Minoxidil: mechanisms of action on hair growth. Br J Dermatol. 2004;150(2):186-194. PMID: 14996087. DOI: 10.1111/j.1365-2133.2004.05785.x
Roberts J, Desai N, McCoy J, Goren A. Sulfotransferase activity in plucked hair follicles predicts response to topical minoxidil in the treatment of female androgenetic alopecia. Dermatol Ther. 2014;27(4):252-254. PMID: 24773771.
Lachgar S, Charveron M, Gall Y, Bonafe JL. Minoxidil upregulates the expression of vascular endothelial growth factor in human hair dermal papilla cells. Br J Dermatol. 1998;138(3):407-411. PMID: 9580790. DOI: 10.1046/j.1365-2133.1998.02115.x
Sato T, Tadokoro T, Sonoda T, Asada Y, Itami S, Takayasu S. Minoxidil increases 17 beta-hydroxysteroid dehydrogenase and 5 alpha-reductase activity of cultured human dermal papilla cells from balding scalp. J Dermatol Sci. 1999;19(2):123-125. PMID: 10098703. DOI: 10.1016/s0923-1811(98)00048-6
Hsu CL, Liu JS, Lin AC, Yang CH, Chung WH, Wu WG. Minoxidil may suppress androgen receptor-related functions. Oncotarget. 2014;5(8):2187-2197. PMID: 24742982. DOI: 10.18632/oncotarget.1886
Pekmezci E, Turkoglu M. Minoxidil Acts as an Antiandrogen: A Study of 5alpha-reductase Type 2 Gene Expression in a Human Keratinocyte Cell Line. Acta Dermatovenerol Croat. 2017;25(4):271-275. PMID: 30064598.
Tang GT, Leemaqz S, Bhoyrul B, et al. Treatment of androgenetic alopecia in transgender people receiving testosterone therapy with sublingual minoxidil: a randomized, double-blind, placebo-controlled clinical trial. J Am Acad Dermatol. 2026 (online ahead of print). PMID: 42140362. DOI: 10.1016/j.jaad.2026.05.020
Elzaghir R, Collins KC, Abdulshafi A, et al. Minoxidil May be a Partial Agonist of Estrogen Receptor Alpha. MicroPubl Biol. 2026. PMID: 42318156. DOI: 10.17912/micropub.biology.002173
Olsen EA, Hordinsky M, Whiting D, et al. The importance of dual 5alpha-reductase inhibition in the treatment of male pattern hair loss: results of a randomized placebo-controlled study of dutasteride versus finasteride. J Am Acad Dermatol. 2006;55(6):1014-1023. PMID: 17110217. DOI: 10.1016/j.jaad.2006.05.007
Kaufman KD, Olsen EA, Whiting D, et al. Finasteride in the treatment of men with androgenetic alopecia. J Am Acad Dermatol. 1998;39(4 Pt 1):578-589. PMID: 9777765.